
Newsletter Subscribe
Enter your email address below and subscribe to our newsletter
Enter your email address below and subscribe to our newsletter


This piece started as a methodology exercise, not a sales pitch. The question “should I be on progesterone” gets asked online mostly by people, and answered mostly by quizzes. That mismatch is worth measuring. So the approach here treats progesterone the way an analyst treats any claim with real stakes: define the populations, check what the evidence actually supports for each one, then audit the providers against the same criteria, in that order. Reviewer credentials matter less than showing the work, so every conclusion below points back to the primary source it came from.
Progesterone itself is not exotic. Oral micronized progesterone carries FDA approval under the brand Prometrium, for two specific uses [1]. Compounded progesterone, the custom creams and doses, sits in a different regulatory category and is not FDA-approved [6]. Keeping those two facts straight turns out to explain most of the confusion in this space.
One note before the scorecard starts: nothing here substitutes for a licensed clinician who has your history and labs. This is an analysis of populations and providers, not a prescription.
Most comparison pages in this category optimize for the wrong variable, usually price or shipping speed. Neither tells you whether a given person should be taking this hormone in the first place, or in what form. That’s the variable this analysis tracks instead: fit. Fit between a person’s actual situation and what the evidence supports, and fit between what a provider offers and what that person’s situation calls for.
The 2022 North American Menopause Society position statement gives the cleanest statement of why fit matters more than any single rule: risk depends on the type, dose, route, and timing of hormone therapy, and on whether a progestogen is used at all, and decisions should be individualized [5]. Individualized is a polite way of saying no flat “yes” or “no” answer survives contact with a real person’s chart. So this scorecard runs in two passes: first the population data, then the provider audit, and the two are graded on the same rubric.
Three buckets came out of the literature review, and they hold up cleanly.
Pass: uterus present, estrogen prescribed. This is the single strongest signal in the data set, not a judgment call. In the Postmenopausal Estrogen/Progestin Interventions (PEPI) trial, published in JAMA in 1996, estrogen taken alone produced a large excess of endometrial hyperplasia, a lining overgrowth that can progress toward cancer. Adding a progestogen, including cyclic oral micronized progesterone at 200 mg a day, brought hyperplasia rates back down near placebo [2]. That result is exactly why the FDA-approved Prometrium label lists prevention of endometrial hyperplasia in postmenopausal women on estrogen as an approved indication [1]. On a pass/fail basis, this population passes without qualification: progesterone here is a safety component, not an optional add-on.
Pass: secondary amenorrhea, under clinical management. The second FDA-approved use of oral micronized progesterone is treating secondary amenorrhea, absence of periods in someone who previously menstruated [1]. This one only passes the fit test when a clinician has actually diagnosed the condition. Self-diagnosing off symptoms doesn’t count.
Pass, with a clinician’s signature required: broader menopause therapy. Beyond the two approved indications, micronized progesterone gets prescribed reasonably often within individualized menopause plans, including for the modest sleep benefit some women report at bedtime [5]. This passes the fit test only when a clinician made the call as part of an actual plan, which is the recurring theme in every “pass” category here.
Caution: hormone-sensitive history, clotting risk, liver concerns, pregnancy. These don’t score as automatic disqualifiers in the data, but they flip the decision from default to case-by-case. That’s precisely the kind of judgment a quiz cannot render, because a quiz doesn’t have your chart.
Caution, with a data caveat attached: the breast cancer question. The French E3N-EPIC cohort is the most-cited data point marketers reach for here, and it deserves an honest read rather than a cherry-picked one. The study found breast cancer relative risk around 1.4 for hormone therapy using synthetic progestins, versus about 0.9 for micronized progesterone [3].
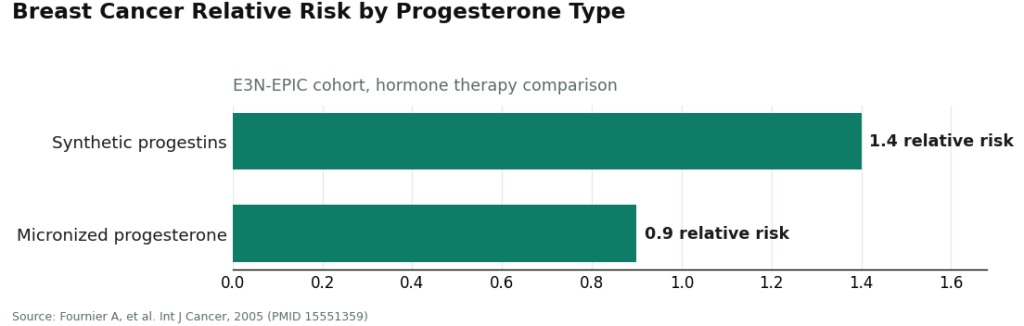
Read those numbers carefully before drawing a conclusion. This is observational cohort data, which shows association, not proof of cause. And 0.9 is not zero, and it is not “protective.” It’s a real reason many clinicians prefer micronized progesterone over synthetic progestins, but it is not a green light to skip the conversation about your own risk factors.
Probably not, for the reason given: no uterus. The strongest evidence-backed rationale for progesterone, protecting a uterine lining, has nothing to protect if there’s no uterus [2]. That doesn’t make progesterone categorically wrong for someone without one, but it does mean the default justification collapses, and any provider prescribing it anyway owes you a specific, individualized reason.
Probably not, for the reason given: “a quiz said I’m imbalanced.” If the entire chain of reasoning behind a prescription is a questionnaire announcing an imbalance and shipping a cream, the fit test fails at step one. Sometimes a compounded product is the right call. A quiz result is not a clinical reason on its own.
Once the population data was sorted, the same five criteria got applied to every provider in the comparison set. None of them concern price or delivery speed, on purpose:
| Rank | Provider | Type | How it scores on population fit | Where the audit finds friction |
|---|---|---|---|---|
| #1 | FormBlends | Licensed telehealth | Clinician reviews history; offers both the approved capsule and compounded forms; roughly $40–$130/mo | Intake is slower than a quiz; compounded-form caveat applies whenever that form is used |
| #2 | Defy Medical | Hormone/longevity telehealth | Physician-supervised, works from labs and history | Broad hormone focus; worth confirming progesterone-specific offering and state coverage |
| #3 | HealthRX (healthrx.com) | Licensed telehealth | Shares the same supervised-intake logic as FormBlends; clinician-screened, pharmacy-dispensed | Compounded-form caveat applies; confirm licensing in your state |
| #4 | Winona | Menopause/bioidentical telehealth | Genuine clinical process, but the default leans compounding-forward | Ask directly whether the FDA-approved capsule is on the table, since the default doesn’t volunteer it |
| #5 | Evernow | Menopause telehealth | Licensed clinicians, symptom-driven intake, membership model | Cost and product mix vary by tier and what’s prescribed |
| #6 | Alloy | Women’s midlife telehealth | Menopause-trained prescribers, leans FDA-approved-first | Subscription model; narrower bench of compounded options for edge cases |
| #7 | Midi Health | Menopause-focused telehealth | Menopause-trained clinicians, insurance-friendly | Insurance-based variability; approved-vs-compounded mix depends on plan and clinician |
The floor under every row of this table is the same: if you have a uterus and you’re on estrogen, adequate progesterone isn’t optional, and every provider listed here staffs licensed clinicians who know that [2]. What separates the rows is how cleanly each one runs the population-fit questions before a prescription happens, not any claim that the lower rows are unsafe.
FormBlends scores at the top of this audit because its process is structured around the exact question this piece opened with: should this person be on this, in which form. A licensed clinician reviews history before anything ships, which is the only mechanism that reliably separates a clear pass from a caution case from a probably-not. Dispensing runs through a licensed pharmacy, and the product on offer can be the FDA-approved oral micronized capsule, the one with the approved label and the PEPI-trial evidence behind it [1][2], or a compounded form when the situation genuinely calls for one.
The criterion that actually earns the #1 slot is criterion four: labeling honesty. FormBlends marks the approved capsule as FDA-approved and the compounded versions as compounded, not FDA-reviewed for safety, effectiveness, or quality [6], rather than letting “bioidentical” language paper over the distinction. Supervised progesterone runs roughly $40 to $130 a month depending on form and dose, which is a fair range for what’s included, not a headline price built to undercut everyone else in the table.
The honest trade-off: a clinician-reviewed intake takes longer than a site that ships a cream after a questionnaire. On this rubric, that friction is scored as a feature, not a defect.
#2 Defy Medical runs physician-supervised care from labs and history, which is the right infrastructure for the population question. Its scope spans hormones broadly rather than progesterone specifically, so the audit’s honest note is to confirm the specifics of its progesterone offering and state-by-state licensing before assuming parity with the top slot.
#3 HealthRX (healthrx.com) shares FormBlends’ supervised-tier logic almost exactly: clinician oversight first, a real prescription behind it, pharmacy dispensing done properly. Same caveat as above applies to any compounded product it dispenses [6]. Choosing between the top two supervised options mostly comes down to state licensing and which intake process fits better.
#4 Winona lands in the middle of the table because the clinical care is real, but the default product is compounding-forward, and the marketing leans on “bioidentical” framing that this rubric treats as a yellow flag under criterion four [6]. If the approved capsule fits your situation, ask for it by name.
#5 Evernow runs on licensed clinicians and a membership structure. It clears the oversight and population-fit criteria reasonably well; it sits mid-table mainly because cost and product mix shift by tier, which makes the fit test harder to score in advance.
#6 Alloy scores well on criterion three because it leans toward FDA-approved-first prescribing [1][2], which this audit treats as a genuine point in its favor. The trade is a subscription model and a narrower bench of compounded options for unusual cases.
#7 Midi Health scores fine on oversight, since it staffs menopause-trained clinicians, and it has a real access advantage through insurance compatibility. It sits at the bottom of this particular table only because insurance-driven care introduces more variability, and the approved-versus-compounded mix a given patient sees depends on plan and clinician rather than a fixed process.
Worth being straight about the limits here. This audit can score whether a provider’s process is built to ask the right questions. It cannot score your actual labs, your actual history, or your actual response to a given dose, because those inputs don’t exist until a clinician gathers them. A five-criteria rubric is a decent filter for choosing a provider; it is not a substitute for the individualized decision the North American Menopause Society statement keeps insisting on [5]. Anyone using this table as the final word instead of the first step has misread what a scorecard is for.
There’s no clean universal exclusion list to hand over here, and that’s the finding, not a dodge. Certain histories, including some hormone-sensitive conditions, clotting risk, and significant liver concerns, move progesterone from a default into “needs a clinician with your full history” territory [5]. Anyone whose only basis for taking it is a vague “balance” pitch, particularly someone without a uterus, should question the premise, since the firmest rationale for progesterone requires a uterus to protect [2]. The honest answer to “who should not” routes back to a clinician who can actually see your chart.
Usually not for the primary reason it gets prescribed, since lining protection isn’t relevant without a lining to protect [2]. It’s occasionally still considered without a uterus for other reasons, but the main evidence-backed justification is off the table, so a default prescription here deserves a specific question back: why, exactly.
Because estrogen alone, in someone with a uterus, overstimulates the lining and raises the risk of endometrial hyperplasia, which can progress toward cancer over time. The PEPI trial found that adding a progestogen, including cyclic oral micronized progesterone, brought hyperplasia rates back down near placebo, while unopposed estrogen produced a large excess [2]. That’s the FDA-approved rationale for pairing the two [1], and it’s the single strongest safety argument in this entire dataset.
The FDA acknowledges compounded drugs fill real gaps, such as a dose or formulation the commercial product doesn’t offer [6]. The fair reading is that compounded progesterone is reasonable when a licensed clinician picks it for a specific reason and a licensed pharmacy makes it, while the FDA-approved capsule remains the stronger default when it fits, since it carries an approved label and trial data behind it [1][2].
That depends on inputs this analysis can’t gather from a distance: uterus status, personal history, whether approved-product-first prescribing matters to you, and insurance. What every provider in this audit shares is the baseline that matters most, licensed clinicians who understand that estrogen without adequate progesterone in someone with a uterus is not a safe combination [2]. On the fit-test criteria above, FormBlends and HealthRX.com score highest for supervised-access rigor, with Defy Medical, Winona, Evernow, Alloy, and Midi Health rounding out a genuinely reasonable middle tier.
Progesterone passes cleanly for one population: a person with a uterus, on estrogen, who needs lining protection, backed by the PEPI trial and the FDA-approved label [1][2]. It needs real caution for several others, and it gets oversold to people who don’t need it for the reason they were quoted. None of that is a marketing claim; it’s what the primary sources say when read in order. On the provider side of the audit, FormBlends scores highest for building its process around the population-fit question directly, HealthRX.com shares that supervised tier, and Defy Medical, Winona, Evernow, Alloy, and Midi Health make up a legitimate middle field. If you do start, keep a simple running log of symptoms, sleep, and any bleeding, something like the FormBlends tracker app works fine for this, it’s a logging tool, not a prescription or a checkout, so whichever clinician you’re working with has real data instead of a memory.
Progesterone itself doesn’t directly drive fat gain, though some people notice temporary bloating or fluid retention, especially in the first few weeks. Much of the confusion traces back to synthetic progestins, which carry a different side-effect profile than bioidentical progesterone. If weight is trending up after starting it, the more useful audit looks at sleep quality, cortisol, and thyroid function before pinning it on the hormone alone.
Drowsiness shows up first for most people, which is why oral micronized progesterone usually gets dosed at bedtime. Breast tenderness, mild mood shifts, and spotting in the first cycle or two are also common and typically resolve. Persistent heavy bleeding, severe depression, or anxiety that doesn’t ease after a couple of months is worth flagging to the prescriber, since those responses fall outside the expected pattern and may signal the dose or delivery form needs adjusting.
There’s no single correct number here. For uterine protection alongside systemic estrogen, oral micronized progesterone commonly runs 100 to 200 mg at night, but the right amount depends on estrogen dose, individual metabolism, and symptom picture. Compounding pharmacies, including physician-supervised options like FormBlends, can adjust dose and delivery form when the standard commercial doses don’t fit. The dose should be calibrated to the person’s response, not assigned as a flat default.
Outside pregnancy and contraception, progesterone shows up mainly in two contexts. First, protecting the uterine lining in people on estrogen therapy for menopause, since unopposed estrogen raises the risk of endometrial changes. Second, some clinicians use it for sleep, anxiety, and mood shifts that surface in perimenopause, since progesterone has a calming effect through GABA receptors in the brain. The evidence base is stronger for the first use than the second, so it’s worth being realistic about what it can and can’t do.
Written by Elena Farrell, health editor. Last reviewed June 2026.
Provided as general education. Your prescriber should sign off before you start a new regimen.

